
 How Stress & Hormonal Imbalances Cause Hair Loss
How Stress & Hormonal Imbalances Cause Hair Loss
Excessive hair loss affects a large portion of the world’s population. Over 25% of women will have female pattern hair loss by the age of 50.1 Male pattern hair loss will affect up to 80% of men and 50% of women during their lifetime, so expect several patients to present to your office with a chief complaint of hair loss.2
While hair loss is not life-threatening, hair loss can negatively impact psychosocial health and quality of life.3,4 Excessive hair loss is known to cause self-consciousness, frustration, jealousy, psychological disturbance, emotional distress, and embarrassment.4
Since hair growth and maintenance are highly affected by free steroid hormone levels – including estrogens, progesterone, cortisol, dihydrotestosterone (DHT), and testosterone – saliva hormone testing is clinically indicated when assessing the underlying cause(s) of hair loss.
 Healthy Hair Growth
Healthy Hair Growth
To understand how hormonal imbalances contribute to hair loss, it is helpful to review and understand how healthy hair grows. Even with optimal hormone levels and robust hair growth, healthy men and women naturally lose 50 – 150 hair strands daily.5,6 Approximately 100,000 hairs are on the scalp in various stages of growth at any single time point.2,7
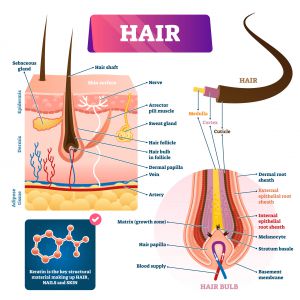
Hair is a filament that primarily consists of dead, keratinized cells. The whole hair structure consists of two main parts: the hair follicle and the hair shaft. The hair shaft is above the skin, while the hair follicle is below the skin.8
Here is an illustration of a hair follicle and hair shaft:
 Each hair undergoes a hair growth cycle that consists of four phases – the anagen, catagen, telogen, and exogen phases, as seen in the image below.7,8
Each hair undergoes a hair growth cycle that consists of four phases – the anagen, catagen, telogen, and exogen phases, as seen in the image below.7,8
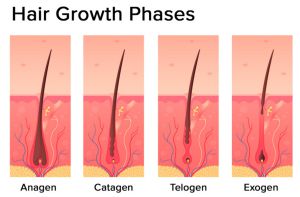 Image source: Hormonal Effects on Hair Follicles
Image source: Hormonal Effects on Hair Follicles
The anagen phase is a growth phase that lasts between 2 to 8 years with an average of 3 years of growth.6,7 Roughly 90% of hairs taken from a normal healthy scalp are in the anagen phase. Proliferation of the hair bulb matrix cells occurs during the anagen phase to produce and lengthen the hair.7
The catagen phase is a transitional phase between the anagen and telogen phases.7 In the catagen phase, all hair growth ceases. Less than 1% of all scalp hairs are in the catagen phase, which lasts for 2-3 weeks.6-8 The telogen phase is a resting phase.7 The telogen phase lasts approximately 2 to 5 months just before the hair falls out, which is known as teloptosis or the exogen phase.6,7,9 Approximately 9% of all scalp follicles are in the telogen phase at any time point in healthy individuals.6
The term “kenogen” refers to the period between the loss of hair and the growth of new hair from the hair follicle.7
 Hormonal Hair Loss – A Change in the Anagen to Telogen Ratio
Hormonal Hair Loss – A Change in the Anagen to Telogen Ratio
Several hormones contribute to healthy hair growth, and hair loss can be caused by an abnormal level of a single hormone or an imbalance in multiple hormone levels. This article will focus on the effects of steroid hormones, including androgens, estrogens, progesterone, and cortisol.
The anagen (growth) to telogen (resting) ratio for healthy subjects is approximately 14:1 to 12:1. Thus, for each hair in the resting phase, healthy individuals have 12-14 actively growing scalp hairs. Hair loss due to hormonal imbalance significantly shifts the ratio.6 In those with androgenetic alopecia (male pattern hair loss), the ratio decreases to 5:1.6 In those with telogen effluvium (TE), which is significant hair loss caused by stress, the ratio decreases to 8:1, leading to hair shedding far above the normal rate of 50–150 strands daily.5,6
 Testosterone, DHT & and Hair Loss – Androgenetic Alopecia (Male Pattern Baldness)
Testosterone, DHT & and Hair Loss – Androgenetic Alopecia (Male Pattern Baldness)
Testosterone, an androgen hormone, is required for healthy hair growth. The overall effect of androgens on hair growth depends on where the hair is on the body. Hair follicles on the face, under the arms, in the groin area, and on the chest are stimulated by androgens.8 Increased production of androgen hormones, including testosterone, transforms the thin, soft “vellus hairs” on the face into the thick, coarse beard hairs known as “terminal hairs” in men during puberty.10 But, high androgen levels tend to inhibit the growth of hair follicles on the scalp.8
Androgen hormones affect hair growth via intracellular androgen receptors in the cells of the hair follicles. The androgen receptors are activated when testosterone and the more potent androgen dihydrotestosterone (DHT) bind to the receptors. The main action of androgen hormones on the hair follicles is the alteration of gene expression that then affects hair growth.8 Androgen hormones are also required to produce sebum, an oily substance that protects the hair. Thus, at optimal levels, androgens tend to stimulate and protect hair growth. However, abnormal androgen levels and activity can lead to male pattern baldness or androgenetic alopecia – one of the most common causes of excessive scalp hair loss.10
 Doctors and research scientists believe male pattern baldness is caused by an imbalance in androgen hormone levels. Specifically, research shows that increased levels of free dihydrotestosterone (DHT) shorten the anagen phase of scalp hair growth.10 Increased androgen levels also impact kenogen.11 Kenogen is the time between a hair falling out and a new healthy hair growing in its place. In a healthy individual, kenogen affects approximately 10% of all scalp hairs and lasts about two months. In men with androgenetic alopecia, kenogen lasts 4–7 months and affects 80% of all hair cycles.11
Doctors and research scientists believe male pattern baldness is caused by an imbalance in androgen hormone levels. Specifically, research shows that increased levels of free dihydrotestosterone (DHT) shorten the anagen phase of scalp hair growth.10 Increased androgen levels also impact kenogen.11 Kenogen is the time between a hair falling out and a new healthy hair growing in its place. In a healthy individual, kenogen affects approximately 10% of all scalp hairs and lasts about two months. In men with androgenetic alopecia, kenogen lasts 4–7 months and affects 80% of all hair cycles.11
Research also suggests that kenogen involves 22% of the hair follicles in women with androgenetic alopecia, and the frequency and duration of kenogen are greater when the hair loss is more severe. In women with androgenetic alopecia who participated in one study, kenogen lasted from 3 months to 1 year.11 Over time, when the anagen phases shorten while kenogen lengthens, the hair follicles shrink and gradually produce shorter, thinner, and softer hairs on the scalp in response to suboptimal or imbalanced free androgen hormone levels.10
Despite modern research advances, many aspects of the influence of androgen hormones on hair follicles are still unclear. Future research studies are required to clarify the varying effects of androgen hormones on hair follicles in all body regions.8
 Stress Hormones (Cortisol) and Hair Loss
Stress Hormones (Cortisol) and Hair Loss
Yes, stress can contribute to and be an underlying cause of concerning hair loss. Telogen effluvium is the medical name for the transient hair loss caused by a significant stressor.12 The stressor could be emotional or physical, such as major surgery or a divorce.
When stress is experienced, the hypothalamic-pituitary-adrenal (HPA) axis responds via the production of several hormones, including corticotropin-releasing hormone (CRH), adrenocorticotropic hormone (ACTH), and ultimately, cortisol, the well-known steroid stress hormone.
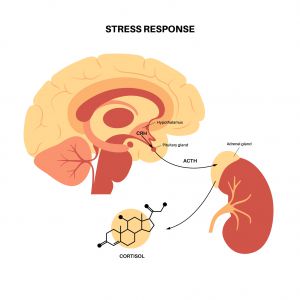 According to research, stress hastens the anagen-to-telogen transition and elongates the telogen phase.6 Corticotropin-releasing hormone (CRH) is the non-steroid hormone released by the hypothalamus to stimulate the function of the entire hypothalamic-pituitary-adrenal (HPA) axis in response to stress. Therefore, individuals under the effects of stress often have high levels of CRH.8
According to research, stress hastens the anagen-to-telogen transition and elongates the telogen phase.6 Corticotropin-releasing hormone (CRH) is the non-steroid hormone released by the hypothalamus to stimulate the function of the entire hypothalamic-pituitary-adrenal (HPA) axis in response to stress. Therefore, individuals under the effects of stress often have high levels of CRH.8
Analysis shows both CRH and CRH receptors are present in the skin, and CRH inhibits hair growth, prematurely stimulates the catagen phase, and reduces the proliferation of keratinocytes, which are the cells that produce the keratin incorporated into the hair matrix. CRH can also alter the expression of genes to affect hair growth.8
As the first hormone released along the HPA axis, CRH also regulates the production of adrenocorticotropic hormone (ACTH) by the anterior pituitary gland. ACTH stimulates the adrenal glands to produce cortisol and androgen hormones. Animal studies suggest ACTH may also induce the anagen phase, but the role ACTH plays in hair growth requires further study and is still unclear.8
 As one of the last hormones produced along the HPA axis, cortisol affects the cyclical regulation of the hair cycle and the synthesis of proteoglycans.6,3 Optimal proteoglycan synthesis is required for healthy hair growth.6
As one of the last hormones produced along the HPA axis, cortisol affects the cyclical regulation of the hair cycle and the synthesis of proteoglycans.6,3 Optimal proteoglycan synthesis is required for healthy hair growth.6
Proteoglycans include decorin and versican. Research shows versican protects cells in the hair follicle from cell death (apoptosis) due to oxidative stress. Decorin promotes hair growth by inducing the anagen phase.6 The high cortisol levels caused by stress can damage the proteoglycans in the hair follicles.6 Cortisol can also indirectly affect hair growth because high cortisol levels decrease the synthesis of insulin-like growth factor (IGF-1).13 IGF-1 is a non-steroid hormone that is the key signal responsible for the stimulation of hair follicle growth.8
Also, men and women with androgenetic alopecia often have higher cortisol levels in comparison to healthy individuals, suggesting both androgens and stress hormones may contribute to the development of male pattern baldness.6 The effect of stress on skin and hair is so significant that Arck et al. proposed a “brain-skin connection” theory to describe the link. The brain and skin, including hair follicles, are affected by many of the same neurotransmitters, neuropeptides, neurohormones, and neuroendocrine-immune interactions.14
Thus, testing and optimizing stress hormone (cortisol) levels and the stress response in your patients may support healthy hair growth.
 Hair Loss Due to Fluctuating Estrogen Levels During Menopause and Pregnancy
Hair Loss Due to Fluctuating Estrogen Levels During Menopause and Pregnancy
Estrogen receptors are expressed locally in hair follicles, so estrogen directly affects hair growth. Estrogen also indirectly affects hair growth via its influence on androgen metabolism since androgens are the precursors for estrogens.8
The most powerful estrogen is estradiol, and research shows estradiol prolongs the anagen phase while decreasing the length of the telogen phase in human scalp hair. When estradiol levels decrease, the transition from anagen to telogen hastens, leading to increased hair loss.15 Two life events that offer insight into the effects of shifting estrogen levels on hair growth are pregnancy and menopause.6
 Postpartum Hair Loss & Thinning (Telogen Gravidarum)
Postpartum Hair Loss & Thinning (Telogen Gravidarum)
During pregnancy, estradiol levels are naturally higher and associated with increased hair diameter, increased hair growth, delayed teloptosis, reduced hair shedding, and a higher anagen/telogen ratio. Hair loss is expected postpartum due to the abrupt decrease in hormone levels. The naturally occurring hair loss after birth is known as postpartum telogen effluvium or telogen gravidarum.8,3
Moms who develop telogen gravidarum note that increased hair shedding begins two to four months after delivery and lasts 6 to 24 weeks. Sometimes, the increased hair shedding can persist for up to 15 months postpartum.8
Many hormonal changes occur during pregnancy, including increased levels of human chorionic gonadotropin, progesterone, prolactin, numerous growth factors, and cytokines, so other hormones may also contribute to the changes in hair growth in pregnant women. Menopause is a life stage characterized by estrogen depletion; thus, it provides more precise insight into the effects estrogens have on hair growth.8
 Menopausal Hair Loss
Menopausal Hair Loss
During menopause, estrogen levels naturally decrease, promoting the miniaturization of the hair follicles in the scalp.1 This estrogen depletion is associated with female-pattern hair loss on the scalp and increased hair growth on the face (facial hirsutism).8 A quarter (25%) of all women are affected by female-pattern hair loss by the age of 50.1
In female pattern hair loss, the frontal hairline of women is often spared, most likely because it has a relatively higher level of aromatase. Aromatase is the enzyme that naturally converts androgens to estrogens. This phenomenon also demonstrates the protective role of estrogen on hair growth.6
When systemic estrogen levels abruptly decrease at menopause, it initiates a cascade of hormonal shifts leading to changes in hair growth in women. One significant change that can occur is a decrease in the sex hormone binding globulin (SHBG) level because estrogen stimulates the production of SHBG.8
SHBG is a blood protein that carries hormones through the blood to distribute them to cells. When a hormone is bound to SHBG, it is inactive. Hormones not bound to SHBG or other blood proteins are known as free hormones. Only the free, active hormones affect the function of cells and tissues throughout the body.
One of the benefits of saliva hormone testing is the direct measurement of the free hormone level. SHBG and other blood proteins are not in saliva, so only the free hormones diffuse into saliva.

The natural decrease in the SHBG level at menopause often causes a clinically significant boost in androgen activity since the free androgen levels, including testosterone and dihydrotestosterone (DHT), tend to increase. The secretion rate of androgens is typically maintained until the later stages of life in women, so an imbalance between estrogen and androgen levels often develops after menopause. The shift in the estrogen-to-testosterone ratio that begins at menopause may drive the decrease in scalp hair growth after menopause, even when the total estrogen and androgen levels are normal.8
It is interesting to note that when total blood levels of androgens are tested in menopausal and premenopausal women, the levels are similar, which is why it is so important to directly test the free hormone levels in saliva instead when there are signs of hyperandrogenism in menopausal women.8
While this exploration of the effects of estrogen on hair growth has primarily focused on women, estrogen replacement therapy has been tested as a treatment for hair loss in male patients, and it was associated with extensive hair regrowth when used in conjunction with other hair loss treatments.6 Changes in free progesterone levels throughout life can also significantly impact hair health.
 Progesterone and Hair Loss
Progesterone and Hair Loss
Research shows progesterone receptors are present in hair follicles, sebaceous glands, and keratinocytes; therefore, progesterone directly affects hair growth. Progesterone also indirectly supports healthy hair growth via its effects on other hormone levels.1
A healthy progesterone level reduces the excessive secretion of Luteinizing Hormone (LH) from the pituitary gland. LH acts on the reproductive organs to increase androgen production in men and women. As noted above, high free androgen levels can cause hair loss, so a healthy progesterone level supports robust hair growth by optimizing LH and androgen levels.8
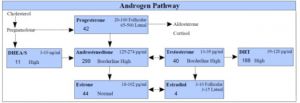
At the level of the hair follicle, progesterone directly decreases the conversion of testosterone to dihydrotestosterone (DHT) by inhibiting the 5-alpha reductase enzyme.8 Therefore, low progesterone levels are associated with high free DHT levels within the hair follicles, which can cause excessive hair loss in men and women.1,8,16
Here are the results of a saliva hormone test panel depicting an elevated free DHT level in a female patient with hair loss:
 Unfortunately, thus far, there are no clinical studies that have assessed the impact of the application of bioidentical progesterone to the scalp on hair quantity and quality in those with excessive hair loss.1
Unfortunately, thus far, there are no clinical studies that have assessed the impact of the application of bioidentical progesterone to the scalp on hair quantity and quality in those with excessive hair loss.1
 How to Stop Hormonal Hair Loss
How to Stop Hormonal Hair Loss
To stop hormonal hair loss, one must determine what hormone, or hormones might be contributing to the hair loss. Saliva hormone testing is the best option for assessing steroid hormone levels because it directly measures the bioactive, free hormone levels. Free hormones are the hormones that are actively affecting cells and tissues throughout the body, including the hair follicles.
Once you assess salivary (free) hormone levels, you can recommend treatment options to optimize hormone levels and balance. One treatment option to consider when a patient’s salivary DHT level is either frankly elevated or high in comparison to their free testosterone or estrogen levels is a natural 5-alpha reductase inhibitor.
5-alpha reductase is the enzyme that converts testosterone to DHT. A natural 5-alpha reductase inhibitor is Saw Palmetto.17 You might also consider assessing and addressing the underlying cause(s) of the increased 5-alpha reductase activity in your patients. For example, insulin resistance is known to increase 5-alpha reductase activity; hence, improving insulin levels and blood glucose management may also reduce an elevated DHT level.18 The Adrenal Stress Index Panel includes tests that screen for insulin resistance.

Other Underlying Causes of Hair Loss
While abnormal steroid hormone levels can cause hair loss, there are many other underlying causes of excessive hair loss, including nutrient deficiencies, autoimmune activity, and exposure to toxic metals, such as thallium, arsenic, mercury, lead, and cadmium. Abnormal levels of non-steroid hormones, which include melatonin, thyroid hormones, IGF-1, and prolactin, may also contribute to hair loss.
If your patients are concerned about hair loss, now is the time to assess and address the underlying cause(s) since some medical conditions associated with hair loss require immediate medical treatment.
 The Best Test Panels for Hair Loss
The Best Test Panels for Hair Loss
Measure salivary (free) steroid hormone levels by ordering a:
- Male Hormone Panel or Expanded Male Hormone Panel
- Adrenal Stress Index Panel
- Customized Flexi-Matrix Panel (Create a customized test panel that combines the Adrenal Stress Index and the Male Hormone Panel.)
- Cycling Female Hormone Panel or Expanded Cycling Female Hormone Panel
- Peri Menopause Hormone Panel or Expanded Peri Menopause Hormone Panel
- Post Menopause Hormone Panel or Expanded Post Menopause Hormone Panel
- Bone Health Panel
Also, consider screening for exposure to toxic metals with a Toxic Metals and Elements Panel.

To place a test order, click here. As a reminder, DiagnosTechs will drop ship test kits directly to your patients. You may select this option at the top of the order form.
Please visit our Provider Tools page for more information about choosing the right test, test result interpretation, and treatment options.
 References:
References:
- Gasser S, Heidemeyer K, von Wolff M, Stute P. Impact of progesterone on skin and hair in menopause – a comprehensive review. Climacteric. 2021;24(3):229-235. doi:10.1080/13697137.2020.1838476
- Piraccini BM, Alessandrini A. Androgenetic alopecia. G Ital Dermatol Venereol. 2014;149(1):15-24.
- Hasan R, Juma H, Eid FA, et al. Effects of Hormones and Endocrine Disorders on Hair Growth. Cureus. 2022;14(12):e32726. doi:10.7759/cureus.32726
- Liu LP, Li MH, Zheng YW. Hair Follicles as a Critical Model for Monitoring the Circadian Clock. Int J Mol Sci. 2023;24(3):2407. doi:10.3390/ijms24032407
- Do you have hair loss or hair shedding? American Academy of Dermatology. Accessed July 28, 2023. https://www.aad.org/public/diseases/hair-loss/insider/shedding.
- Natarelli N, Gahoonia N, Sivamani RK. Integrative and Mechanistic Approach to the Hair Growth Cycle and Hair Loss. J Clin Med. 2023;12(3):893. doi:10.3390/jcm12030893
- Saleh D, Nassereddin A, Cook C. Anagen Effluvium. [Updated 2022 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482293/
- Grymowicz M, Rudnicka E, Podfigurna A, et al. Hormonal Effects on Hair Follicles. Int J Mol Sci. 2020;21(15):5342. doi:10.3390/ijms21155342
- Rebora A, Guarrera M. Teloptosis and kenogen: two new concepts in human trichology. Arch Dermatol. 2004;140(5):619-620. doi:10.1001/archderm.140.5.619
- Martel JL, Miao JH, Badri T. Anatomy, Hair Follicle. [Updated 2022 Oct 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470321/
- Guarrera M, Rebora A. The Higher Number and Longer Duration of Kenogen Hairs Are the Main Cause of the Hair Rarefaction in Androgenetic Alopecia. Skin Appendage Disord. 2019;5(3):152-154. doi:10.1159/000493587
- Kesika P, Sivamaruthi BS, Thangaleela S, et al. Role and Mechanisms of Phytochemicals in Hair Growth and Health. Pharmaceuticals (Basel). 2023;16(2):206. doi:10.3390/ph16020206
- Kraemer WJ, Ratamess NA, Hymer WC, et al. Growth Hormone(s), Testosterone, Insulin-Like Growth Factors, and Cortisol: Roles and Integration for Cellular Development and Growth With Exercise. Front Endocrinol (Lausanne). 2020;11:33. doi:10.3389/fendo.2020.00033
- Wang Q, Wu H, Zhou J, et al. Involvement of the central hypothalamic-pituitary-adrenal axis in hair growth and melanogenesis among different mouse strains. PLoS One. 2018;13(10):e0202955. doi:10.1371/journal.pone.0202955
- Lephart ED. Human scalp hair: Modulation by various factors and hormones do estrogens inhibit or stimulate-A perplexing perspective. J Cosmet Dermatol. 2019;18(6):1860-1865. doi:10.1111/jocd.12888
- Thom E. Stress and the Hair Growth Cycle: Cortisol-Induced Hair Growth Disruption. J Drugs Dermatol. 2016;15(8):1001-1004.
- Devjani S, Ezemma O, Kelley KJ, et al. Androgenetic Alopecia: Therapy Update. Drugs. 2023;83(8):701-715. doi:10.1007/s40265-023-01880-x
- Sadgrove NJ. The new paradigm for androgenetic alopecia and plant-based folk remedies: 5α-reductase inhibition, reversal of secondary microinflammation and improving insulin resistance. J Ethnopharmacol. 2018;227:206-236. doi:10.1016/j.jep.2018.09.009